Heritability: what it
means for genetic ALS

Genetic ALS / Heritability
4 min read
C9orf72: one piece of the genetic ALS puzzle
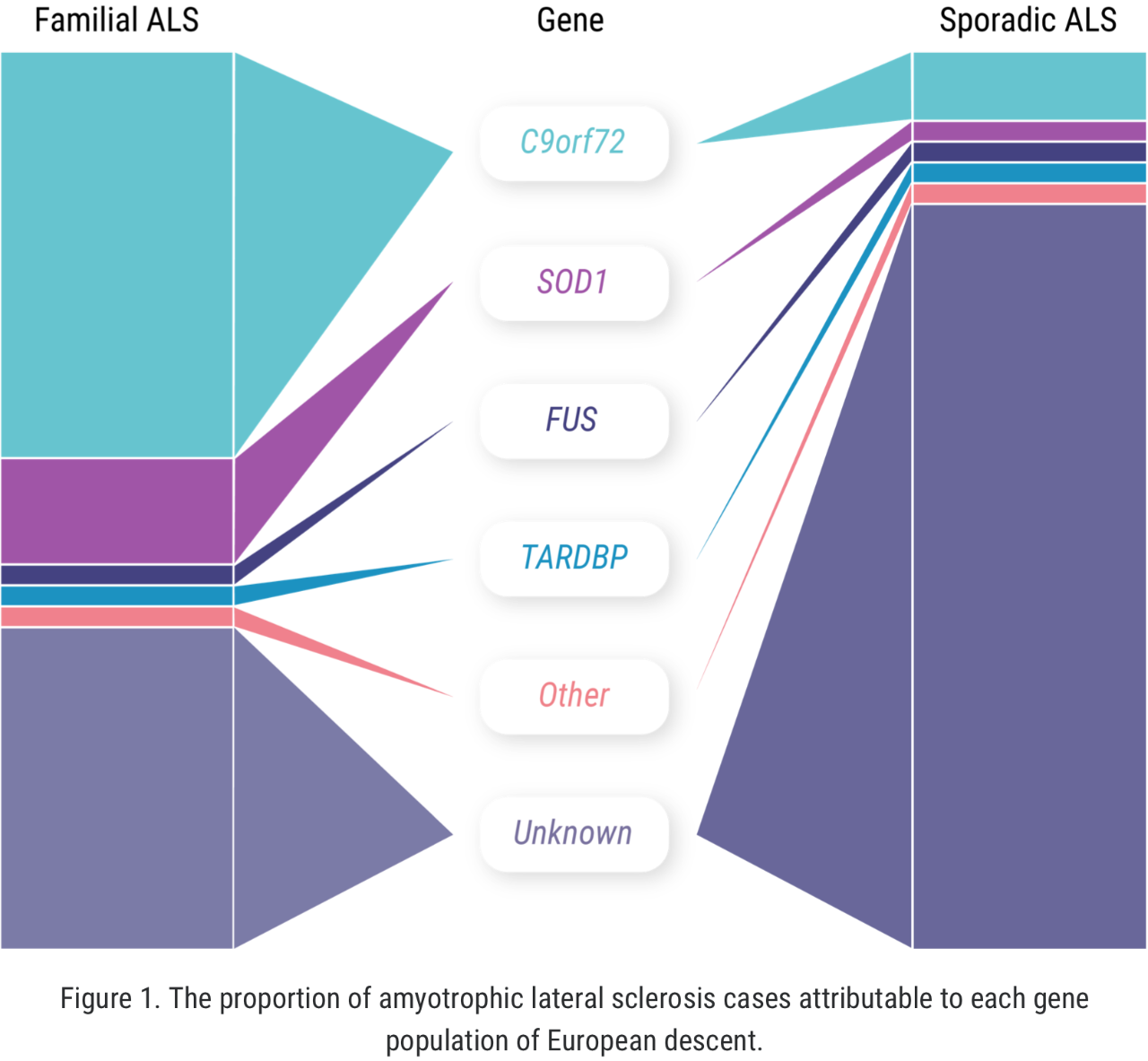
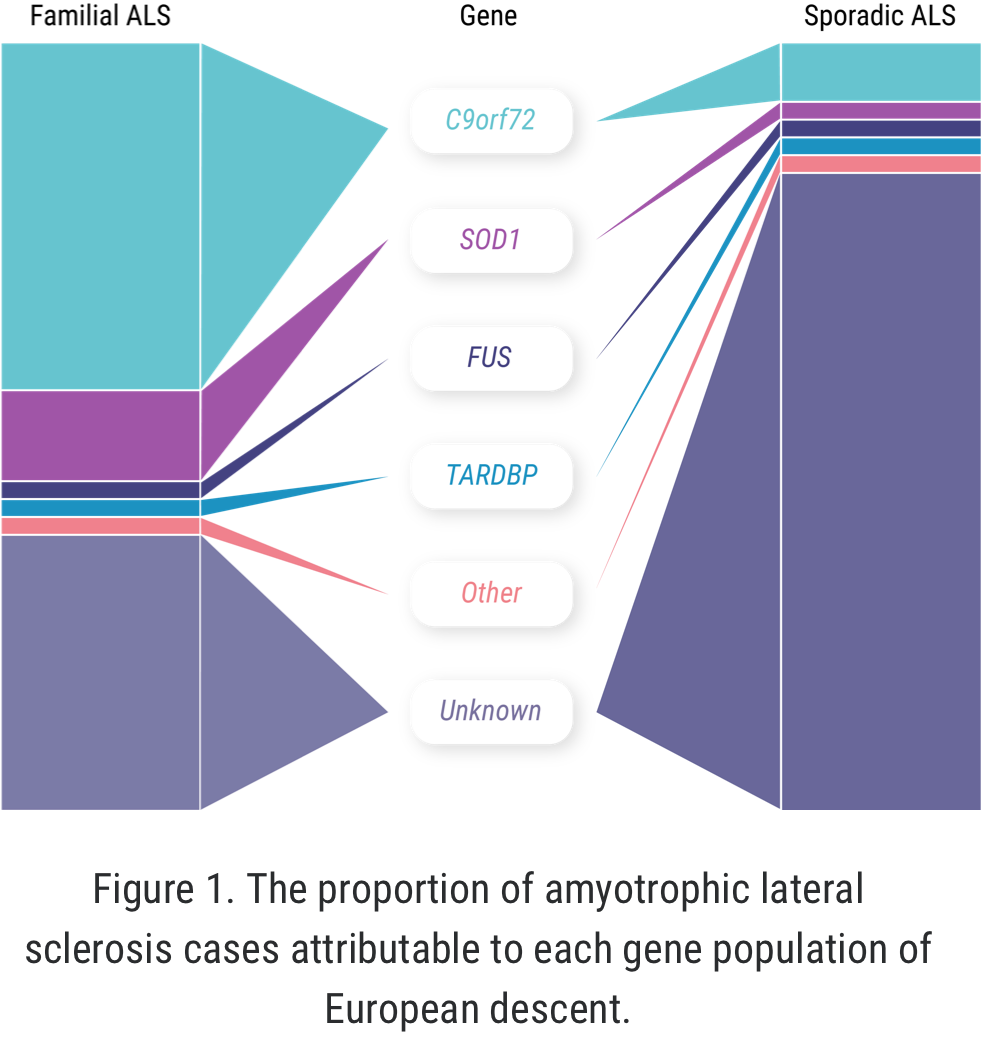
When it comes to C9orf72 and ALS, Professor Orla Hardiman and her team at Trinity College sought to uncover the role of the gene itself, independent of other factors. C9orf72 is the most common gene mutation associated with ALS, affecting 6% to 10% of all patients with ALS of European descent; this includes approximately 41% of all familial ALS and 8% of all sporadic ALS.7,8
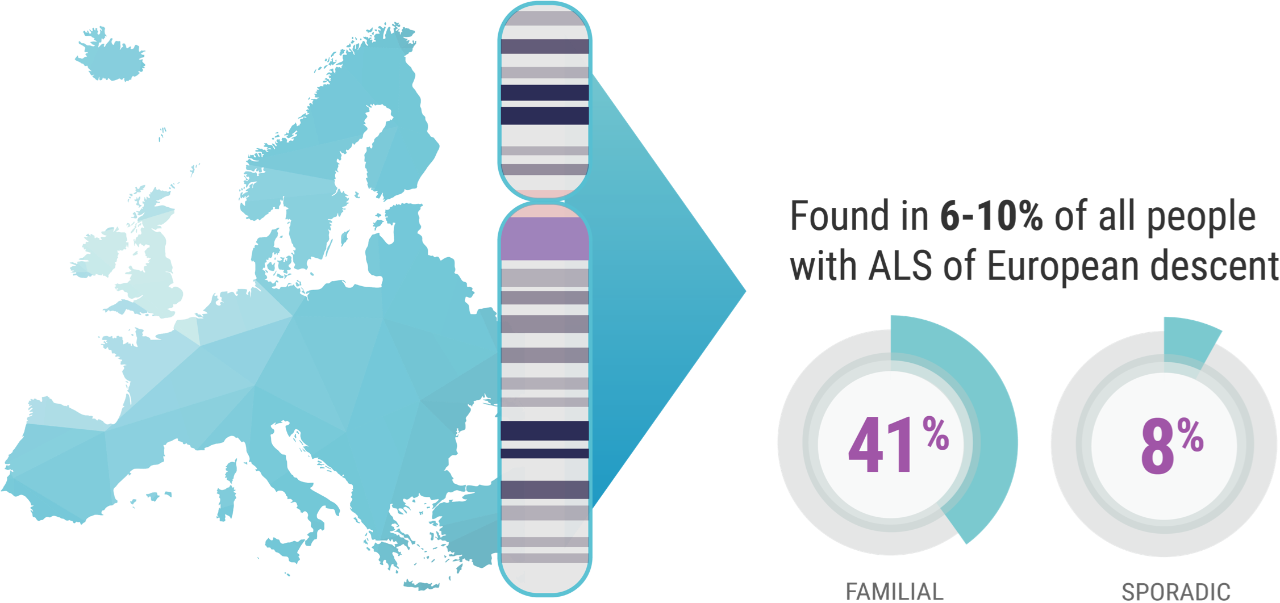
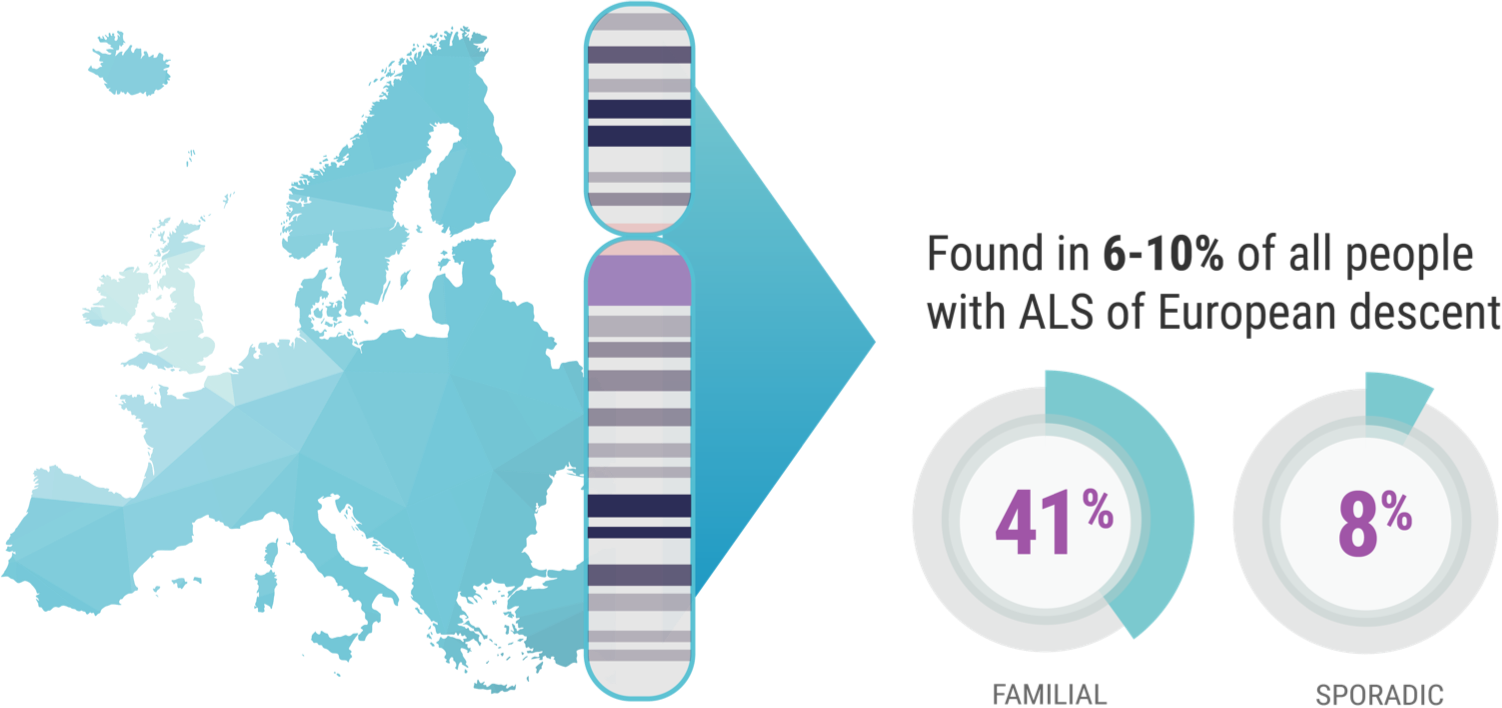
Professor Hardiman’s study focused on patients in Ireland who have ALS and the C9orf72 genetic mutation. “And we know,” continued Prof. Hardiman, “for example, 10% of patients in Ireland carry the C9orf72 variant,9 which is just a bit higher than the rest of European-descended populations. So, it's relatively common in Ireland.”
Although SOD1-ALS is the second-most common form of genetic ALS worldwide, no cases have been identified in the Republic of Ireland to date, though cases have been reported in Northern Ireland. Hence, Hardiman and her team focused on C9orf72 as there were no cases of SOD1-ALS in Ireland to investigate.9,10
The study, which looked at parents with C9orf72-ALS and their children, suggested that the presence of the C9orf72 gene mutation was an important determinant of lifetime risk, or the odds of whether a child would develop ALS. This is not to say that having a parent with C9orf72-ALS is a guarantee the child will develop ALS. We still don’t know the true rates of transmission of C9orf72-associated ALS from parents to children.9
According to the team’s research, the lifetime risk of developing ALS for first-degree relatives of individuals with the disease was approximately 1.4% compared with the general population. This is higher than individuals without a first-degree relative with ALS, for whom the rate was approximately 0.3%.9
ALS varies from case to case, based on factors outside of genetic mutations present.11 Hence, the researchers’ second goal was to find out whether the C9orf72 mutation itself contributed to the effect of other factors.
The other pieces of the genetic ALS puzzle
The Trinity College research suggested that gender played a role: the mean lifetime heritability for all patients involved in the study was 52.3%, but this figure rose to 66.2% when considering mother-to-daughter pairings.9 But Prof. Hardiman noted that, beyond these other factors, understanding the genetic impact tied to ALS within a population is important information for researchers such as herself.
“That's a very positive thing in a sense, because if we can understand why that is, or what the patterns are that lead to depressive degeneration, then we're very much on the pathway towards better understanding the disease,” she explained. That understanding relies on identifying more detailed subgroupings of ALS patients to better understand all the factors that play into the complex equation that is the disease’s development, and how it varies from case to case.
Sex-specific heritability estimates by overall heritability
cohort and C9orf72-negative subcohort
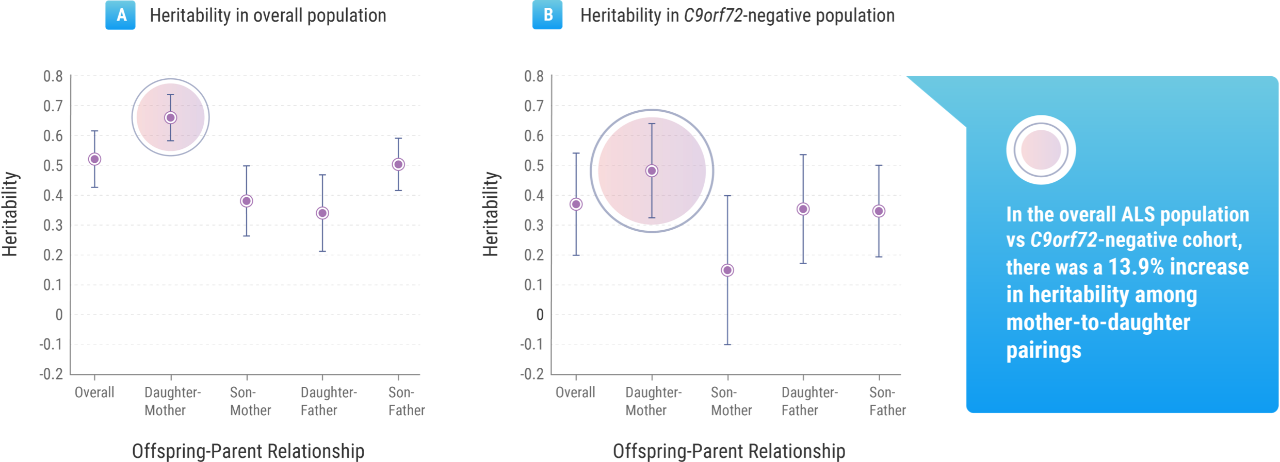
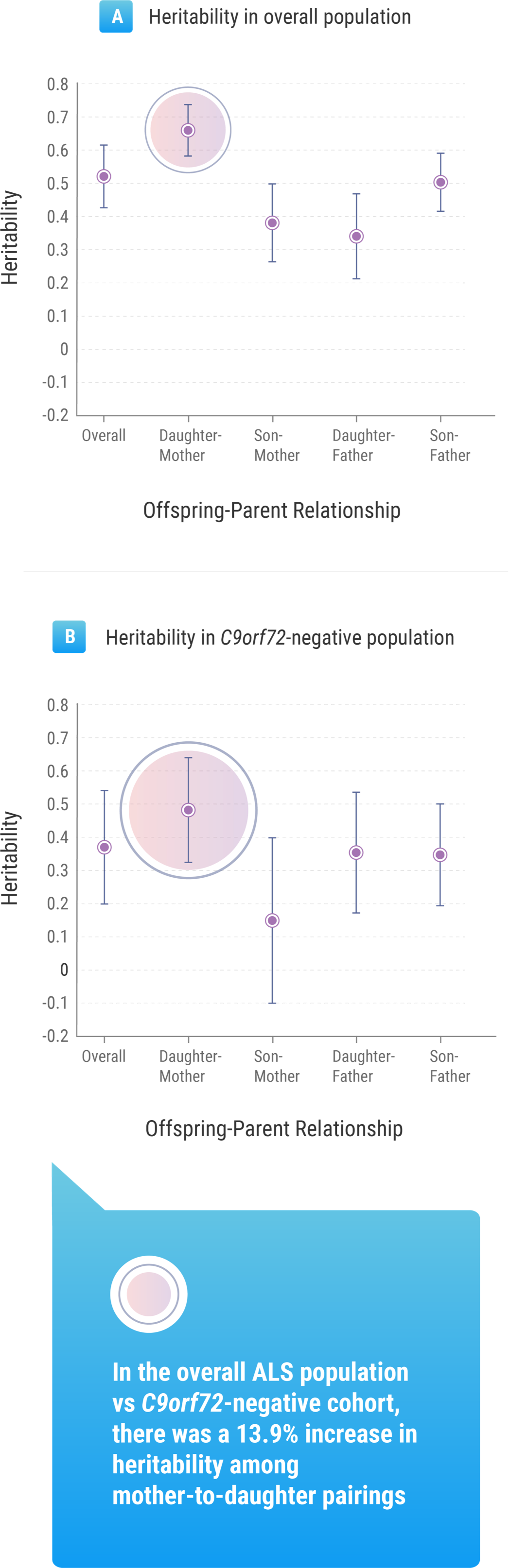
Adapted from Ryan M, et al 20197